

In our shoulders we want to achieve freedom and stability in the shoulder girdle allowing us to move pain free in our everyday lives, not lock it down and cause more tension in the body.
As an ex swimmer I have struggled with my shoulders for years. I ended my competitive swimming career with rotator cuff surgery. Even after physical therapy it wasn't until I found Pilates that I was truly able to rehabilitate my shoulders. Below is a very brief introduction to what is shoulder stabilization and some of the issues it can cause in our bodies if we are unable to achieve it. This text was part of a shoulder girdle workshop I did in 2017.
Brief Anatomy Overview
The Shoulder is a muscle dependent joint. Therefore we need to focus on strengthening the muscles around the joint for proper function of the joint.
We will be focusing on the muscles around the scapula (the stabilizers) and also the rotator cuff, which are largely underused and weak in most of us. The back extensors will also play a large role in this approach in this workshop. Of course, I believe in a highly integrated approach - no one joint or muscle is acting alone. It is part of a system and in Pilates we are working to achieve balance within our own system. The shoulder joint is a very mobile joint. Mobile joints equal unstable joints. However we want to be sure we are preserving, if not enhancing, the mobility of the joint, not locking it down. The key is to connect and strengthen the muscles that will allow the bones to move in their intended design.
The shoulder girdle is made up of a pair of clavicles and scapulae with the only bony attachment to the axial skeleton via the clavicle at the sternoclavicular joint. The shoulder joint is a ball in socket joint but it is very shallow to allow greater mobility than other load bearing joints (e.g. hip) that need more stability. The humerus sits in the glenoid fossa at the edge of the scapula. (Think golf ball sitting on a tee)
This region can be broken into three muscle groups - scapular stabilizers, rotator cuff and the large shoulder muscles.
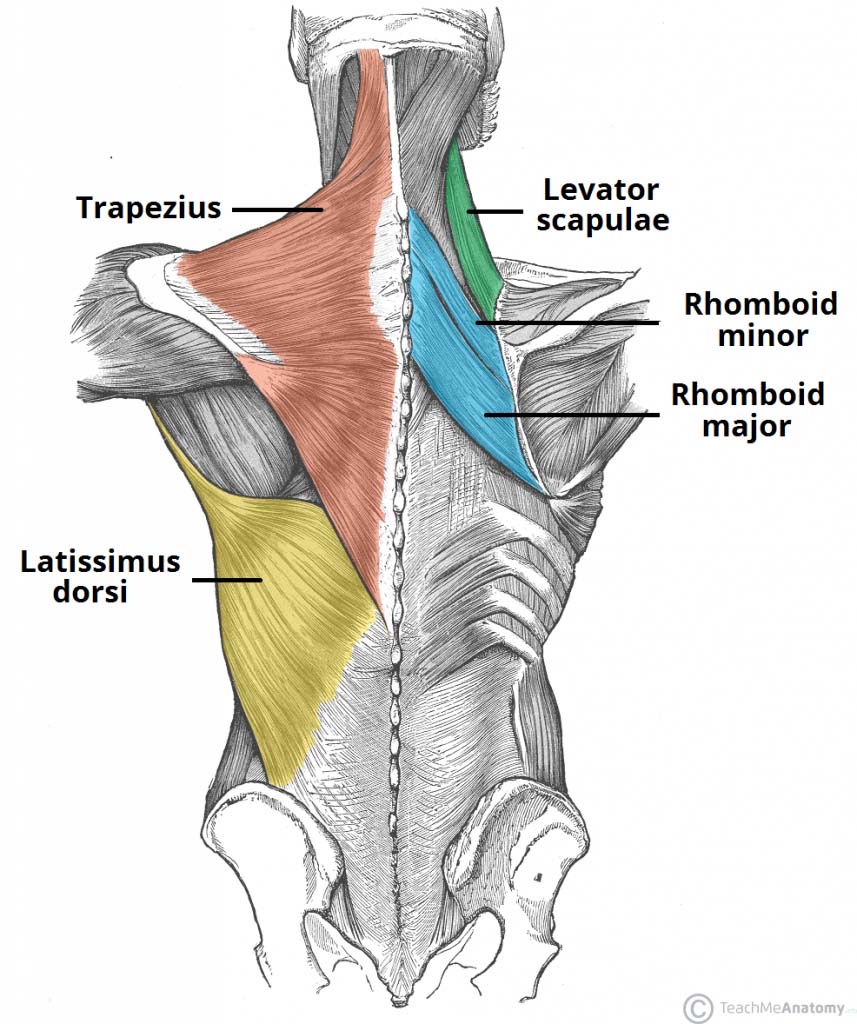
The scapular stabilizers connect the scapulae to the surrounding bones (skull, spine, rib cage) but do not have a direct connection to the humerus. The primary function of these muscles is to stabilize or move the scapulae in accordance with the needs of the arm. These muscles are the trapezius, rhomboids, levator scapulae, pectoralis minor and the serratus anterior.
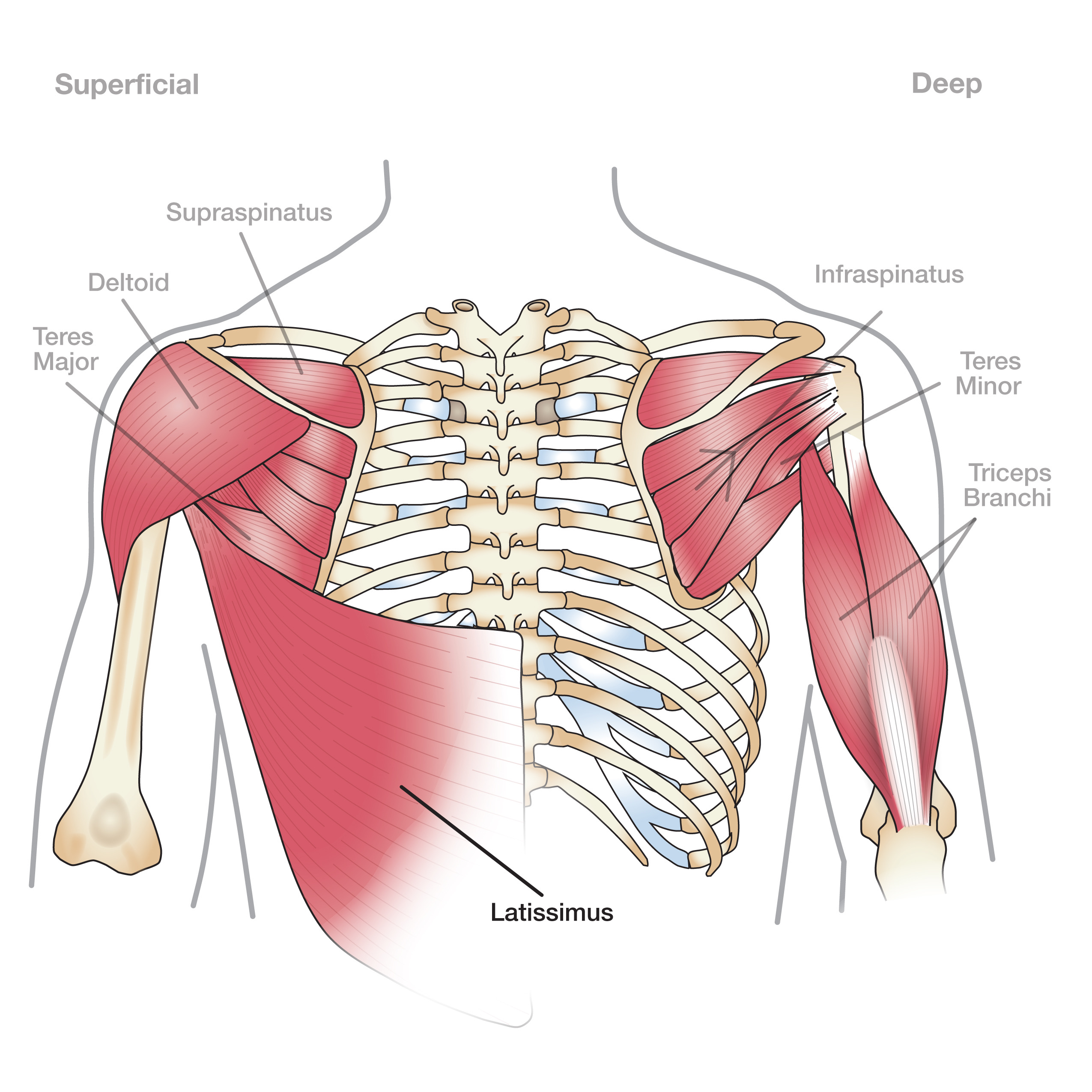
The rotator cuff is a group of small muscles that connect the scapulae to the proximal humerus. The rotator cuff provides stability to the shoulder joint proper and facilitates subtle mechanics of the shoulder. These muscles are the supraspinatus, infraspinatus, teres minor and subscapularis
The large muscles of the shoulder produce gross movements of the arms. These muscles are pectoralis major, deltoids, latissimus dorsi and teres major.
Correct shoulder mechanics involves a coordination or linked movement of the scapula and humerus called scapulohumeral rhythm. The stabilization of the scapula provides a base upon which the arm can function correctly.
Restrictions, Compensations, Injury
If there is a restriction in the body, it compensates, which leads to injury.
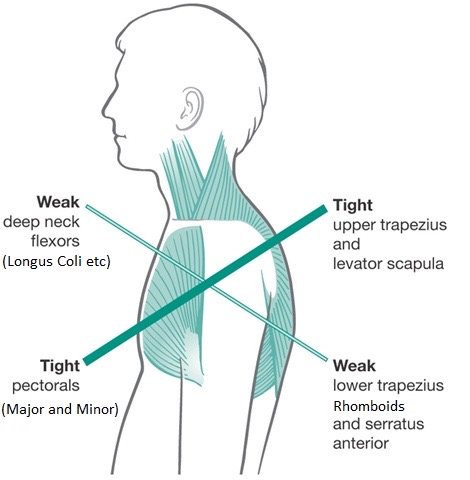
Restriction - Without proper alignment and mechanics, problems can occur in the shoulder or related areas such as the back and neck. Our forward lifestyles (working at a computer, driving, caregiving) and well as sports (swimming, cycling, golf) shortens our pectoral muscles in the front of the girdle, it narrows the shoulders with the shoulder joint pulled forward, as well as, causing kyphosis in our thoracic spines. When this happens the scapula cannot “hang” freely and glide. They become fixed which prevents the arms from working correctly. Therefore it is just as important to stretch the front of the girdle as it is to strengthen the back to acheive balance back in the body.
Compensations - If there is a restriction in the shoulder girdle other parts of the body start to compensate and vice versa. These compensations can come in the form of improper recruitment of shoulder muscles or affect other joints and muscles in our body, such as the head and neck falling forward, the pelvis can also fall forward to compensate for a kyphotic spine.
Injury - If alignment and balance is not returned to the body injuries within the shoulder girdle will start to form. Below are common pathologies of the shoulders.
- Round shoulder syndrome
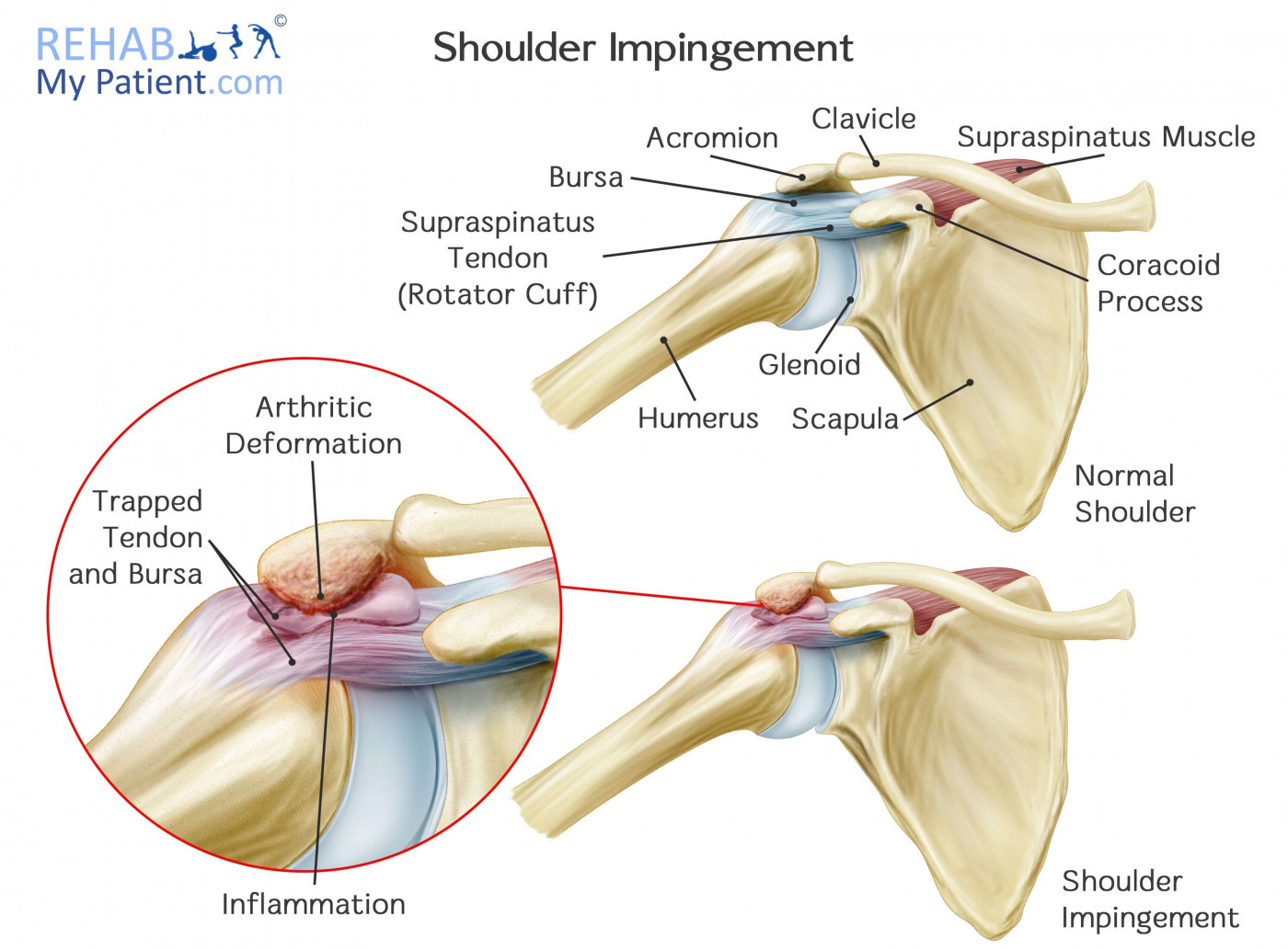
- Impingement syndrome
- Rotator cuff tendinopathy (overuse injury)
- Rotator cuff tear
- Neck pain and headaches (overuse of the upper trapezius)
- Thoracic outlet syndrome (nerve impingement)
- Shoulder instability or dislocation
- Tendonitis (inflammation of the tendons)
- Thoracic outlet syndrome
Stabilization for Greater Mobility
This is the goal! We don’t want to lock down our shoulder joints and further limit their mobility. We want to free our shoulders and allow them to work as intended (or as close to that as we can get). It’s about balance we don’t want our shoulders to round forward nor squeeze back. We don’t want to elevate the scapula nor over depress them. They should float somewhere in the middle of the girdle and we want to glide and rotate across the rib cage to allow for optimal mobility within it’s proper range.